Case Study : Treatment presbyopic with mixed hyperopic astigmatism and hyperphoria with PALs.
By dr.loft ,O.D.
public : 22 November 2023
Introduction
Today, the cold wind visits Bangkok people after a long absence. However, it is not sure how long it will stay but What’s for sure is that the PM2.5 will follow soon. While the weather is still good, let's take a deep breath before the promotion season starts but We don't have to worry about the frame and lens promotion, because we will see it throughout our lives (just kidding). Let's get to the point.
This case is not difficult. The main knowledge used is the accuracy of refraction and the collection of small scales of binocular dysfunction but If you don't check bionic, you won't know. If you don't know, you won't fix it. And sometimes even though the patient doesn't complain ,it’s not mean you can skip bionocular function test and maybe the patient think you don’t know enough to ask so be quite is more polite than ask someone who don’t know anything but just can sell the glasses.
Case History
The case today is about a 46-year-old male patient who came to clinic with the following symptoms:
- His current progressive lenses, which he has been using for 3 years, are still clear for distance, but not for near vision.
- He is in good health, has no underlying medical conditions, and does not take any medication regularly.
- He uses a computer for 6 hours a day.
Clinical Findings
Acuity (VASC): OD 20/100 OS 20/150
Retinoscopy:
OD +0.25 -3.00 x 90 ,VA 20/20
OS +0.25 -3.00 x 90 ,VA 20/20
Monoc. Subjective Refraction (SRx):
OD +0.25 -2.50 x 83 ,VA 20/20
OS +0.00 -3.50 x 93 ,VA 20/20
Subjective Refraction (SRx):
OD +0.25 -2.50 x 90
OS +0.25 -3.50 x 90
VACC : OU 20/15+2
Binocular Function (w/SRx): 6 m 40cm
Phoria 1.5 EP 5XP’
Base-in (BI) vergence X/5/2 -
Base-out (BO) vergence - -
Vertical Phoria 0.5 BDOD - (right hyperphoria) w/ Vongrafe’ technique
0.5 BDOD - (right hyperphoria) w/ Maddox rod
Associate phoria Horz-Ortho
BCC - +1.50D
NRA/PRA (rely bcc) - +0.75/-0.75D
Fine tune on trial frame w/ handeld JCC.
refraction
OD +0.25 -2.25 x 83
OS +0.25 -3.12 x 87
Phoria : 1.00 BDOD -right hyperphoria (with Maddox rod method)
Ocular Health : normal
Trial Frame: Patient felt comfortable at all viewing distances with the subjective refraction data.
Assessment
1. Mixed hyperopic astigmatism OD and OS
2. Right hyperphoria
3.presbyopia
Treatment Plan
1. Rx: OD +0.25 -2.25 x 83
OS +0.25 -3.12 x 87
2.prism Rx : slits vertical prism : 0.5BDOD/0.5BUOS
3.Rx : progressive additional lens w/ Add +1.50D
Discussion
Mild hyperopia
In terms of vision, it was found that there was mild hyperopia (hyperopia) in both eyes. Even if it is slight, but it must be corrected. Otherwise, it will become a burden on the focusing system. As a result, the lens of the eye is stimulated to focus all the time. When the focusing force (amplitude of accommodation) is reduced due to having to compensate for looking far away, the focusing force for looking near is reduced.
This leads to over addition. And as you know, the more add, the more distortion, the narrower the structure of progressive lens. In addition, the dynamic of the focusing/relaxing system will be reduced. It makes it impossible to relax or focus to change the clear distance by itself. they have to bend down and look up to find the clear distance on progressive lenses instead. This lowers the ergonomic in life, neck pain, and headaches.
High astigmatism
In terms of astigmatism, the patient has a high degree of astigmatism. The DNEye scan, which is used to see the shape of the eye's lenses, found that the patient has astigmatism in both the cornea and the lens.
The important point to remember about astigmatism is to not be afraid of full correction. Do not believe in the myth of “don’t full astigmatism correction" because it is a hoax. However, you must be sure that the amount of astigmatism you find is accurate. But If you do not use a retinoscope, do not be confident that you can find the correct amount of astigmatism. This is because 0.25 diopters of uncorrected sphere can change the amount of astigmatism by 0.50 diopters and axis changed, too. Therefore, trusting subjective refraction and making it up is too rough for working at the level of an optometry clinic.
In addition, as I have often mentioned, the distortion that occurs on progressive lenses is actually the amount of astigmatism that we put in to make the layers of the progressive lens homogeneous (unwanted oblique astigmatism). This is well designed, with parts that are usable (visual field) and parts that are not usable (distortion).
When we under/over correct astigmatism, it will cause the amount of astigmatism that is caused by our incorrect measurement, whether it is the matter of tilting the axis into the main axis-meridian (180/90 degree) or changing the amount of astigmatism lens to something else, it will be combined with unwanted oblique astigmatism in progressive lens structure, which can be additive or subtractive.
It will destroy the ideal-original structure that is designed to be different. When the visual field in each eye is different, it will not be symmetrical. When it’s overlay non-symmetrical visual fields, they will never overlap perfectly. It will make the visual field narrower again, making it difficult to use in real life. And this is the main reason why the progressive lens structure is narrow.
Explain more about distortion on progressive lens
the distortion that occurs on progressive lenses is caused by the amount of astigmatism that is used to make the layers of the lens homogeneous. This astigmatism is called "unwanted oblique astigmatism" because it is not the type of astigmatism that is desired for clear vision.
if the amount of astigmatism correction is not correct, it can cause problems with the visual field of the progressive lenses. This is because the visual field of each eye will be different, and the visual fields will not overlap perfectly when the eyes are aligned. This can make it difficult to see clearly at all distances. And this is the main reason why the structure of progressive lenses is narrow. This is because the structure of the lens is designed to minimize the amount of distortion. If the amount of astigmatism is not correct, it can cause the structure of the lens to be wider to accommodate the different visual fields. This can make the lenses more difficult to use and can also reduce the quality of vision.
to responsible.
For those who are responsible (teacher on university), do not teach student about modifying astigmatism correction. Do not use phrases while you be consult in clinic such as…
…”The patient has never worn astigmatism before, can he wear it?" Or "This is a lot of astigmatism, have you checked the patient's habitual previous astigmatism ,yet?” Or "could he adapt to this oblique-axis of astigmatism? Or “Have you tried adjust it into the main axis (180/90, yet)?” Or “Astigmatism power between two eyes are different like this, it is difficult to adapt ,Have you tried making it the same ,yet? Or “If you reduce the astigmatism on one side and it is not clear, you just add negative or reduce positive sphere ." …
All these recommend are almost to ignore of astigmatism correction, should not recommend to do. You just tell the truth and teach them about the reason why people can easy adapt or hard adapt to these kind of refractive error and how to minimize these aberration by physic-science lens technology not by art of modifying prescription.
However, some people may say that they have tried full correction, but the patient cannot walk. In this case, go back to the previous paragraph and ask yourself if you are sure that the prescription is correct. Have you used a retinoscope to perform over refraction to get a neutral light ,yet? Have you used a handheld JCC to fine-tune the astigmatism, yet? If you have not done all of these steps, do not be sure that the prescription is full.
If you have done all of these steps and the patient still cannot walk, the ground may be uneven or the patient may be feeling dizzy. In this case, check the type of trial frame or trial lens that you are using. There are two types of trial lens sets: biconcave/biconvex (two-sided concave or convex) and corrected curve trial lens set or meniscus lens (always convex on the front and concave on the back).
This is the importance of making sure that a prescription is correct before saying that it is full. Another word is that if a patient is still having difficulty walking after trying full correction, then the prescription may not be correct. If you sure that your prescription is corrected , the type of trial frame or trial lens that is being used may be a factor in the patient's difficulty walking. And this is about each type of trial lens set.
Trial lens set
There are two type of trial lens sets that are available , Bi-concave /convex trial Lens set and meniscus corrected curve trial Lens set.
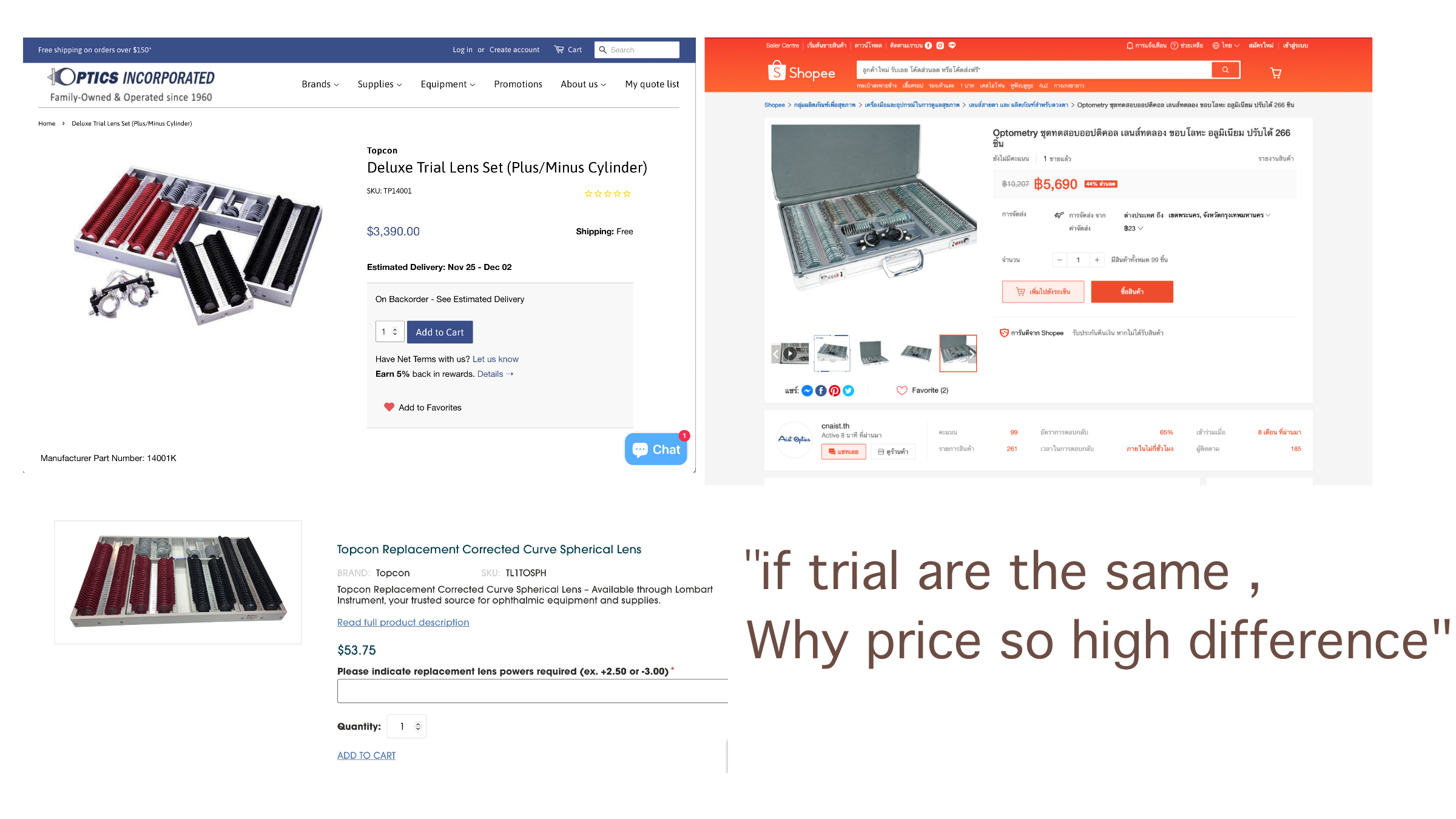
The left image is a meniscus corrected curve trial lens set. The price is $3,390 or about 120,000 Thai baht (excluding import duty) and is sold separately for $53 or about 2,000 Thai baht per piece. The right image is a biconcave/biconvex trial lens set of 266 pieces. The price on Shopee is around 5,000 baht, including delivery, and no additional taxes are required. Why is the price of these two items so different, even though they have the same function?
If you have a patient with severe vision problems wear the lenses in the right image, will they be able to walk? Then you choose to reduce the value, reduce the astigmatism, and ignore the astigmatism degree to reduce aberration, just because your equipment is not up to standard? Is that it? And you will still teach your studen to modify prescription prescribe glasses so that they can wear them? I think this is a joke that happens in developing countries.
The first type, biconcave/biconvex, is the most common type. It is made from low-quality glass and has poor aberration control. This means that it can cause problems for patients with high prescriptions, especially when walking.
The first type (biconcave/biconvex) is available from Chinese sets for 4,000 baht to Japanese sets for 27,000 baht. The only difference is the quality of the lens glass, but the aberration control is equally poor, especially in high prescriptions. The patient can only see at the center, and if the trial frame does not have a center control, the patient will not be able to control the center and will experience dizziness when walking.
Think about it for a moment. Have you ever seen a prescription lens that is convex on both sides or concave on both sides? The answer is no. And if you do, do you think you can wear it? It is impossible to wear it. So why are trial lens sets like this was made?
The answer is that they are made for vision testing, not for real-life use. It is no wonder that most people who use this type of lens set have problems with patients who cannot walk after trying them on, especially with cylindrical lenses. This is because cylindrical lenses are concave on both sides and can cause dizziness when walking. This leads to the practice of using less astigmatism power to let the patient can walk (because the aberration is reduced). However, this will reduce the clarity of vision, resulting in over minus, which is the formula for success in the science of vision correction.
the poor aberration control of biconcave/biconvex trial lens sets is due to the fact that they are designed for vision testing, not for real-life use. When a patient is being fitted for glasses, the trial lens is held in place by the trial frame. This helps to control the center of the lens and prevent aberration from occurring. However, when the patient is walking, the trial lens is not held in place and can move around. This can cause aberration and lead to dizziness.
it is not surprising that many patients who use biconcave/biconvex trial lens sets have problems with dizziness when walking. The author also suggests that this type of trial lens set should not be used for real-life use or trial walking.
The second type is meniscus trial lens. In this type of trial lens set, each lens is ground to match its base curve. This is because of the physics of base curve effect, which states that each prescription has a single base curve that is optimal for it. If the base curve does not match, it can induce base curve effect, which can lead to unwanted oblique astigmatism. This sounds familiar, doesn't it? It is the same phenomenon that occurs on progressive lenses.

Meniscus corrected curve traial lens set : Macro corrected curve trial lens set + Oculus UB4 and UB6 ,that i use in my practice.
Therefore, this type of lens is essentially a lens that is made to match the prescription exactly. The front surface is always convex, regardless of the prescription, and the back surface is always concave, regardless of the prescription. This means that the aberration is low, and the patient will not feel dizzy when walking. This is because the light from all directions is focused at the same point, and there is no distortion. The patient will not feel any problems, even if the trial frame does not hold the center of the lens perfectly. The lens will still perform well, and the patient will not have to be fitted.
The price of this type of trial lens set is approximately 3,500 USD, or about 150,000 baht in Thai currency. However, when it arrives in Thailand, it will probably be increased by another 100,000 baht. The top-of-the-line model from Oculus is priced at around 245,000 baht.
Here are some additional details about meniscus trial lens sets:
- This type of trial lens set is made from high-quality glass and has good aberration control.
- It is a better choice for patients with high prescriptions or who are prone to dizziness.
- It is more expensive than biconcave/biconvex trial lens sets, but it is a worthwhile investment for patients who want the best possible experience when trying on glasses.
In summary about the two types of trial lens sets:
- Biconcave/biconvex: This type of trial lens set is made from low-quality glass and has poor aberration control. It is the most common type of trial lens set and is available from a variety of manufacturers.
- Corrected curve: This type of trial lens set is made from high-quality glass and has good aberration control. It is more expensive than biconcave/biconvex trial lens sets, but it is a better choice for patients with high prescriptions or who are prone to dizziness.
Trial Frame
Trial frames are also available from Shenzhen, ranging in price from hundreds to tens of thousands of bath. The one I am using is about an Oculus UB4, which costs $850, which is about 30,000 baht in Thai currency (if it is sold in Thailand for about 45,000). The price may be high, but it is necessary if you are working in a detailed scale.
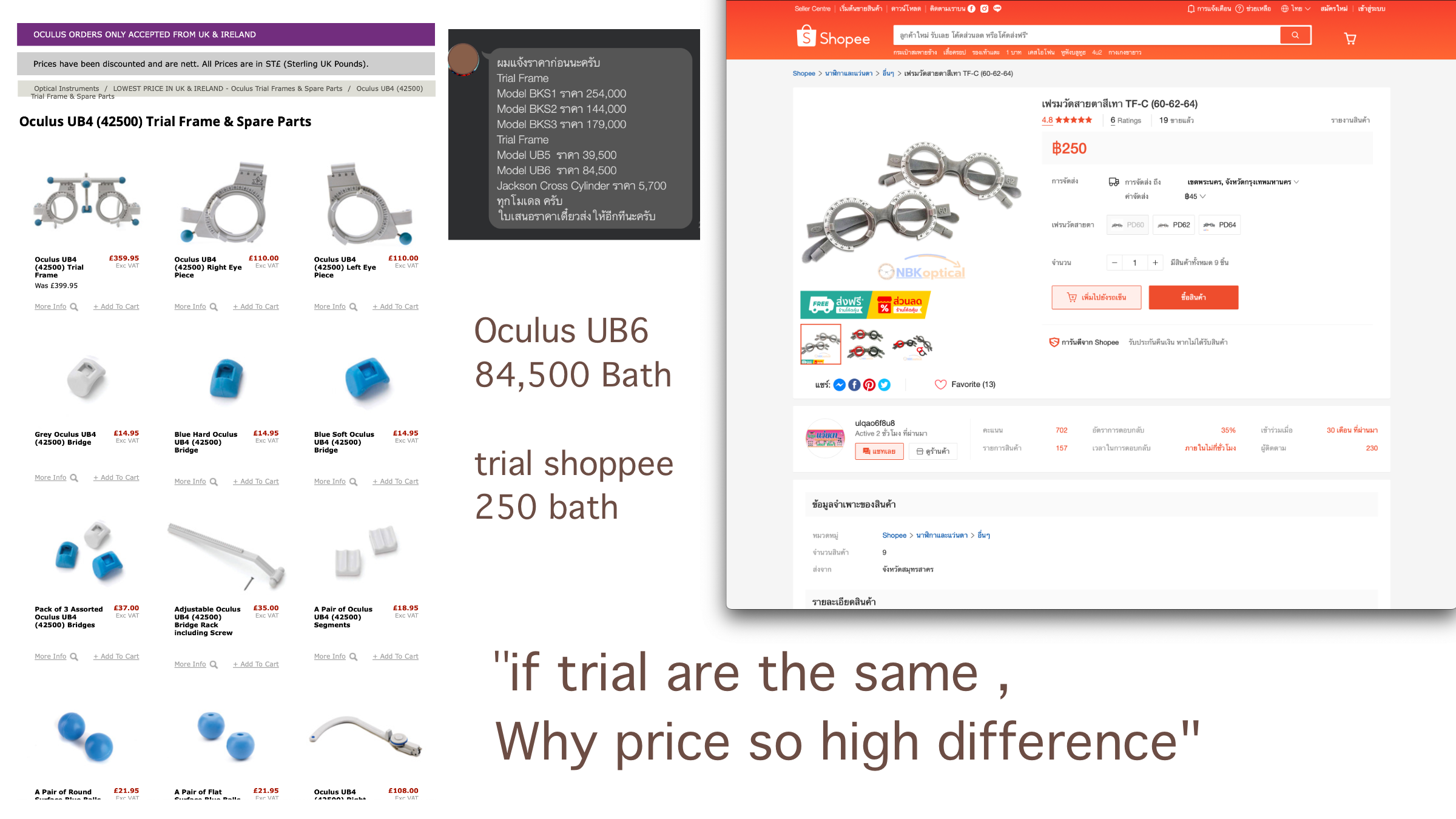
Oculus trial frames are 338 times more expensive than trial frames from Shopee. This begs the question: why? Is it worth the investment? It depends on what each person values. Some people can't bring themselves to buy expensive tools, even if they are essential for their profession, but they can easily buy an iPhone 15 Pro Max without a second thought. That's the difference mindset make difference work value.
Hypothetically, if the examination is detailed, the tools are good, the trial lens set / trial frame is the best, the patient can walk well, but the patient cannot wear it when it is prescribe for, then I would like to say here that "the lens that is paid out is not good enough." Therefore, in addition to knowledge of optometry, knowledge of lens technology should also be available. Do not assume that all clear lenses from any brand are the same.
Therefore, for the past 10 years, I have never modifying patient prescription to another from what’s I’ve test and never had any problems. Therefore, this science of (not) knowledge (to modify prescription to be another) has never been true, but it is strange that it is still taught and passed on. But they also refuse to do detailed scales. The retinoscope is not used. Just Autorefractometer-shooting and then trial in a set of Chinese low quality lenses, then saying that full correction is really not possible.
All this is not a problem for me with people who are studying, but I have a problem with the teachers in school of optometry . Why don't you teach the truth? Let the children use the truth to be of real benefit. I often emphasize that the science of modifying prescription makes the optometry profession under develop. Because even a grandmother of dinosaur can do it this way and she doesn't have to study hard for 6 years. Then we study for 6 years. Seriously, will we copy the technique of a grandmother like that?
The Phoria
Horizontal Phoria
From the examination of the binocular function, it was found that the eye had a slight latent inward angle (1.5BO) from the examination by the vongrafe's technique. There is BI-reserve : x/5/2 but found to be orthophoria with the associate phoria examination technique. I think it is possible that the patient wore too much minus because the original lens used was a myopic lens. The lens was over-stimulated continuously for a long time, which may be the reason why the binocular function may be a bit messy. And I believe that after corrected well, it should make the system return to normal.
Vertical Phoria
In terms of vertical phoria, it was found that there was a latent angle of the right eye floating higher than the left eye, oscillating at 0.5 prism on the phoropter, which was confirmed by both vongrafe's technique, maddox rod and associate phoria. And when tested free space on the trial frame, it got the value at 1.00 prism (R-hyper). Then, I let the patient look at VA through the correction with prism and pull out the prism to see the difference. The patient reported that if not wearing the letters will be stacked and riding each other, making it difficult to distinguish small letters. And let's try walking, don't feel strange. It's the end of the latent angle correction, which the technique is not difficult, but you just have to understand what you are looking for, why you are doing it, and how you are doing it.
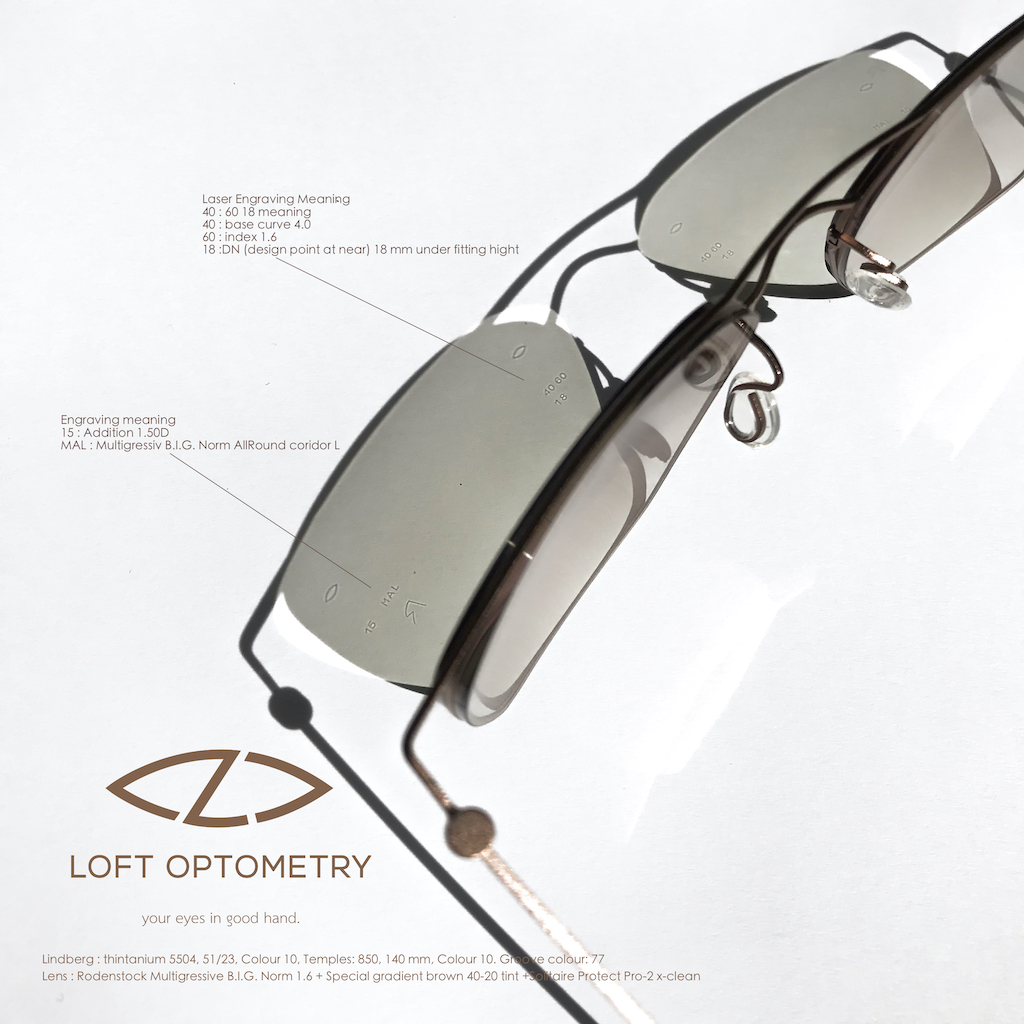
Progressive lens Rx
Lens: The lens used is Rodenstock Multigrssiv B.I.G. Norm 1.6 w/ special color gradient chestnut brown (40%-10%). This is a mid-range lens with a quality that far exceeds its price. Compared to the quality of general market lenses, the technology is considered to be superior to the top models of all brands. And this model, from experience, has no reject. If anyone pays and rejects, start with the issue of vision that can be examined , fitting, centering, and parameter. And this lens model does not require the value of vision that has been modified. If it is modified incorrectly, it should not be blamed on the lens.
Conclusion
If you choose to walk on the path of optometry, you should not be afraid or create fear of prism. Instead, you should learn it to understand it thoroughly, from understanding the physical characteristics and functioning of the visual system, to understanding the abnormalities of the system in a comprehensive manner. Don't just memorize it to take the exam and then throw it all away after test.
In you do only refraction but throw away all binocular function test like optician done, but the truth is your refraction still not good because it is still use modified prescription technique . You will be not difference form dinosaur grandma sells glasses in optical shop.
If this is the case happen, what weapons will optometry have to fight against them? Promotions? How much cheaper will it be? Can you beat the thousand-branched chain optical shop ? It's clearly a toothpick trying to pry a log. Don't do it. So sharpen the sword in your hand. Start with the teacher to understand yourself first. Every weapon has a way to use it. If you don't know or don't understand, go back to the manual. Don't be afraid of yourself, then teach others to be afraid. Like being afraid of a tiger, so you drew a tiger in paper to be afraid of yourself, and then told student to be afraid of a paper tiger.
Optometry is a medical science. Therefore, everything can be proven, checked, and backed up or cross-checked. Because the truth is only one truth, it can be nothing else. Unlike art, which is anything. It can be a world-class artist like Ajarn Chalermchai, or a LoSo like Ajarn Mai Rom. It can be said that an artist creates art. The difference is what kind of art the world recognizes and what kind of art the world does not endorse.
Art in optometry should be about providing knowledge and understanding of the side effects of treatment with each lens model that is paid for. Teach how to cope and adapt. Set a clear learning and adaptation time. Have a clear treatment goal. Don't just upgrade the lens models. Ex. If you upgrade to the top and you still don't get it, what will you do? Move to a different lens brand? If you move to all brands, where will you move to next? If that happen there are two ways: make your own brand lenses or move to a new store to find new customers. Go around like a snake eating its own tail.
Summary
In the conclusion, optometry is a science with some an art. So optometry should be based on evidence and that it should be able to be verified. An optometry should be about providing patients with the best possible care, not just about making money.
Go back and ask yourself what your true reason for studying optometry was. What is the reason for opening an optometry clinic? But if it is for money, then you will suffer on your journey in the optometry profession for a long time. Because if you put money first, you will miss the details of the case. Your knowledge will be like a frog's tai . A frog's tail grows back if it is lost, but it is never as long or strong as it was before. In the same way, an optometrist who puts money first will eventually lose their passion for the profession and their knowledge will become outdated. So the older you get, the dumber you get. In the end, you will be worthless, and how can something worthless have value?
"leave it to think." and Thank for your reading ,See you next time.

Dr.Loft ,O.D.
make an appointment
578 Vacharapol rd, Tha-rang ,Bangkhen ,BKK10220
Mobile : 090-553-6554
Line id : loftoptometry
maps : LOFT OPTOMETRY MAPs
facebook : www.facebook.com/loftoptometry
facebook : www.facebook.com/loftoptometry.eng
Product
Lindberg : thintanium 5504, 51/23, Colour 10, Temples: 850, 140 mm, Colour 10. Groove colour: 77
Lens : Rodenstock Multigressive B.I.G. Norm 1.6 + Special gradient brown 40-20 tint +Solitaire Protect Pro-2 x-clean