Case Study
Topic : Blur and Diplopia cause of compound myopic astigmatism with Right Hyperphoria and exophoria.
Story by : dr.loft,O.D.
Public : 14 October 2023
Preview Case
The case I will be sharing with you today is called "Blur and Diplopia Cause of Compound Myopic Astigmatism with Right Hyperphoria and Exophoria.”Another word, it means "The patient sees blurred images due to myopia and astigmatism, problems seeing up close due to presbyopia, and double vision due to latent strabismus."
Here is a brief summary:
The patient is a 50-year-old man who came in with the complaint that his current glasses were clear for both near and far vision, but he saw double images. He had to cover one eye to make the double images go away. When he tried to focus on something without seeing double images, he had to concentrate very hard, but the double images would come back soon after. If he looked at something very far away, he would not feel the double images (which is caused by the brain suppressing one eye and using the other eye to see, a mechanism that the body uses to adapt to the problem). This problem had been present since childhood.
The examination revealed the following visual system abnormalities:
- Far vision: Myopia and astigmatism, which caused blurry vision without glasses
- Near vision: Presbyopia, which caused blurry vision up close
- Double vision: Latent strabismus, which caused double images when wearing the patient's original progressive lenses
The solution to all of these problems, which had been present since the patient could remember, was a single pair of lenses. The patient was able to fuse the images immediately after putting them on. He could see depth, clarity, and a 20/15+2 binocular vision, which is better than the standard and something he had never been able to do since childhood. He also did not feel that the aberrations on the progressive lenses were a problem or interfered with his vision. This is a very interesting case, so I wanted to share it with you today.
Case History
A 50-year-old man presented with the complaint of blurry distance vision due to myopia. He also reported double vision when wearing his current glasses, both at near and far distances. This problem had been present since childhood. He currently wears progressive lenses that he has had for 3 years. He has double vision when looking at near objects and has to close one eye to make the double vision go away. He does not see double vision when looking at distant objects (due to suppression).
The patient is otherwise healthy and does not take any medications other than general vitamins. He uses his eyes for general activities, including using a mobile phone, tablet, and driving.
Preliminary eye exam
Visual acuity with correction (VAcc): 20/20 in both eyes, but with double vision
Visual acuity without correction (VAsc): 20/200 in both eyes, but with double vision
Cover test (with habitual refraction): Right hyperphoria and high exophoria at both near and far distances
Refraction
Retinoscopy:
OD -2.75 -0.75 x100 VA 20/20
OD -2.50 -0.50 x70 VA 20/20
Monocular subjective:
OD -2.00 -0.75 x93 VA 20/20
OD -2.50 -0.75 x80 VA 20/20
While performing binocular vision assessment (BVA), which is a procedure to balance accommodation between the two eyes to determine visual acuity (VA) while looking with both eyes, the patient was unable to fuse the images and saw double vision. Therefore, the BVA was skipped and binocular function was assessed first.
Functional ; (Vergence and accommodation) at distant 6 m.
Worht-4-dot : Diplopia (R-hyper and exo deviate)
Horz.phoria : 6.5 BI (exophoria)….., w/ VonGrafe’s technique
: 5 BI ,Exophoria …..,w/ Associate phoria
Vertical Phoria : 6.5 BDOD ,Right Hyperphoria ….., w/ VonGrafe’s technique
: 8.0 BDOD ,R-hyperphoria …. ,w/ Maddox rod
: 6.5 BDOD ,R-hyperphoria …. ,w/ Associate phoria
: 6.5 BDOD ,R-hyperphoria …. ,w/ Maddox in free-space trial
After obtaining the prism power that allows the patient to fuse the images, which is 6.5 BDOD (r-hyper) and 6.5BI (exophoria), the prism is placed on the phoropter. Then, Worth-4-dot is used to ensure that the patient can fuse the images. Then, BVA is performed again.
BVA: w/ prism correction 6.5BDOD/6 BI
OD -2.00 -0.50 x108
OS -2.00 -1.25 x60
VAOU: 20/15+2
Functional at Near 40 cm
Horizontal phoria : 12 BI, exophoria
Vertical Phoria : 7 BDOD, Right-hyperphoria
BCC : +2.00D (w/ prism correction 6.5BDOD/6 BI)
NRA/PRA : +0.75D/-0.75D (w/ prism correction 6.5BDOD/6 BI)
Note: Some people may wonder why BI, BO reserve is not done. It is unnecessary for this case because the patient cannot fuse the images from the beginning. It is not useful to do this measurement, it is a waste of time, it is better to focus on other things.
Explanation:
The text describes the results of a binocular vision assessment. The patient was found to have a vertical phoria of 7 BDOD (right hyperphoria) and a horizontal phoria of 12 BI (exophoria). These were corrected with prisms of 6.5 BDOD and 6.5 BI, respectively.
The patient's best-corrected visual acuity (BCVA) was 20/15+2 in each eye. The patient was able to fuse the images with the prisms in place, as confirmed by the Worth-4-dot test.
The note at the end of the text explains that it was unnecessary to perform BI and BO reserve measurements. These measurements are used to assess the ability of the eyes to converge and diverge independently. In this case, the patient was unable to fuse the images without prisms, so it was clear that they had a problem with convergence or divergence. Therefore, performing BI and BO reserve measurements would have been a waste of time.
Assessment
1.compound myopic astigmatism OD and OS
2.Right Hyperphoria
3.Exophoria
4.Presbyopia
Plan
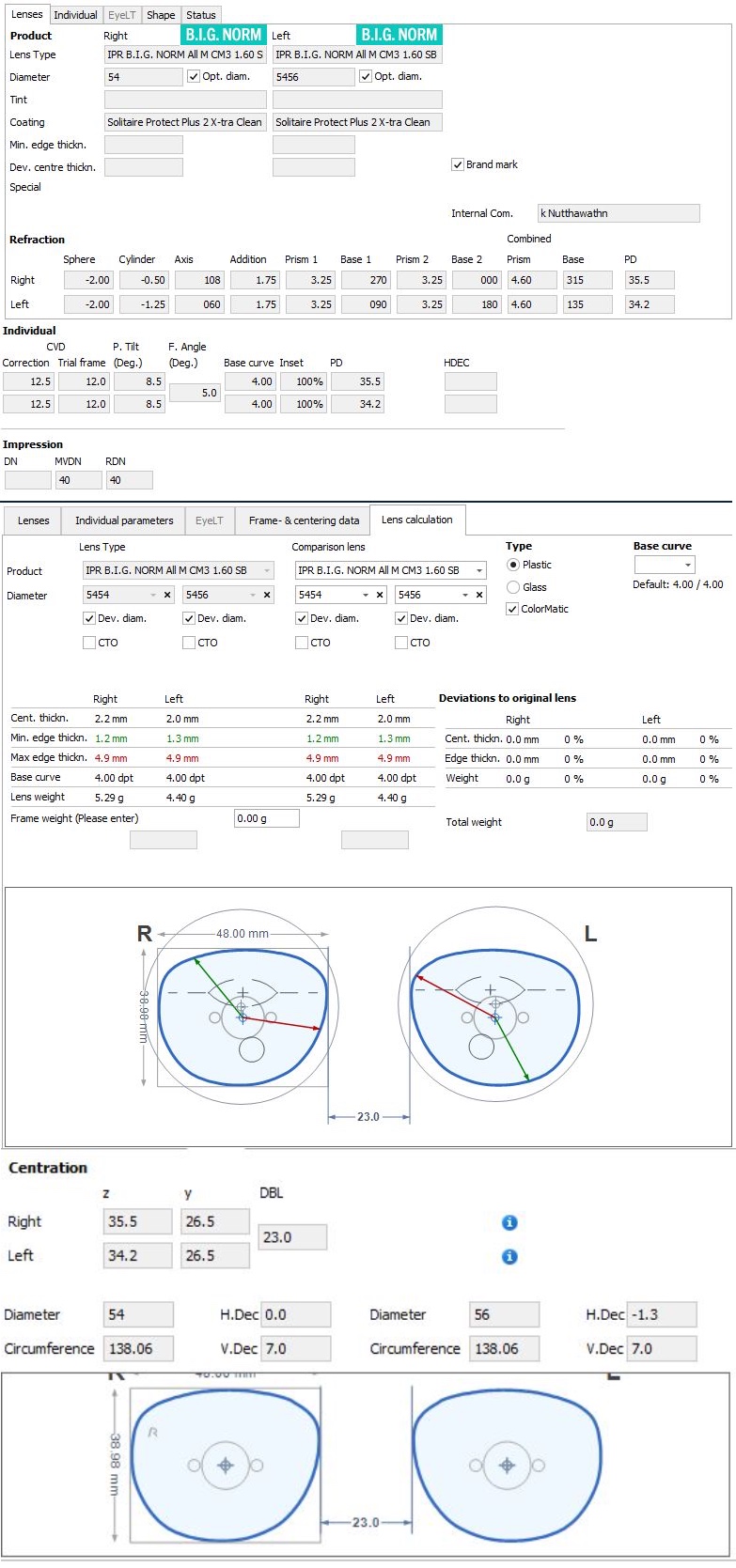
1.Full Rx
OD -2.00 -0.50 x108
OS -2.00 -1.25 x60
2. Vertical prism rx : 3.125BDOD /3.125BUOS
3. Horizontal prism rx :
4.Addition Rx : +2.00D
5.Vergence facility training : 6BI/12BO vergence facility training
Optical Treatment
Lens : Rodenstock Impression B.I.G. Norm 1.6 CMIQ BlueGray ,plus2 x-clean
Frame : Lindberg titanium rim ,Max custom spec
Outcome
The patient was able to fuse the images immediately after receiving the new prescription. He reported that he had no double vision at all and could see clearly with both eyes. He was very happy with the results.
Discussion
This case is an example of a patient with compound myopic astigmatism and latent strabismus (phoria). The patient's original glasses were not able to correct the latent strabismus, which was causing the double vision. The new prescription was able to correct both the myopic astigmatism and the latent strabismus, which resulted in the patient being able to fuse the images and see clearly with both eyes.
Analysis
This case is not particularly difficult from a refraction or addition standpoint. The patient has typical myopia and astigmatism, as well as presbyopia due to age. However, simply prescribing glasses would not have improved the patient's quality of life, as the chief complaint was double vision.
Binocular Dysfunction and Stereopsis
Humans are predators, and as such, our eyes are located in the front of our skulls to allow for binocular vision. This allows us to perceive depth, which is essential for tasks such as hunting and driving.
In this case, the patient had latent strabismus, which was causing the double vision. The new prescription was able to correct both the myopia and astigmatism, as well as the latent strabismus. This resulted in the patient being able to fuse the images and see clearly with both eyes.
Limits of Lens Prescriptions
There is a limit to how much prism can be prescribed in a lens. The manufacturer cannot prescribe more than 10 prism diopters. This meant that the doctor had to prioritize the vertical prism, as the body is not designed to compensate for much vertical misalignment.
The doctor was able to correct the vertical misalignment completely, but there was still some horizontal misalignment. The doctor prescribed the maximum amount of prism possible to correct this misalignment.
The doctor also recommended that the patient do exercises to strengthen the eye muscles. This would help the patient to fuse the images more easily and for longer periods of time.
Frame Selection
The prism in the lenses made them thicker than normal. This meant that the doctor had to choose a full-frame frame to accommodate the thickness. The doctor also chose a small frame to minimize the weight of the lenses.
Conclusion
This case is a good example of how binocular vision can be improved with the right prescription and exercises.
Additional Benefits of Binocular Vision
In addition to depth perception, binocular vision also provides the following benefits:
- Increased visual acuity
- Improved contrast sensitivity
- Reduced eye strain
- Reduced risk of accidents
Conclusion
Binocular vision is essential for many everyday tasks. It is important to have your eyes examined regularly to ensure that you are getting the most out of your vision.
Depth Perception
Stereopsis is the ability to perceive depth by comparing the slightly different images from each eye. This is done by the brain, which compares the visual angles of the images to create a three-dimensional image.
We can try this by closing one eye at a time. We will see that the wide image we see with both eyes at the same time is made up of images from each eye that have different visual fields. The temporal field of each eye sees a wider area than the nasal field. However, there are also areas of the nasal field that look similar. The brain believes that the images it sees are the same, so it sends signals to the eye muscles to force the eyes to look at the same thing. This causes the two images to overlap, and the brain then interprets the difference in the angles of the images as depth.
We can also try listening to a stereo speaker system with one ear, and then with both ears. We will notice that the sound is much flatter and less immersive with one ear. This is because the brain is not getting the same information from both ears, which is necessary to create a sense of depth.
The same is true for our eyes. Stereopsis is essential for many everyday activities, such as driving, walking down stairs, reaching for objects, playing sports, and even eating.
Benefits of Stereopsis
- Improved visual acuity: Stereopsis can improve visual acuity by helping the brain to focus the eyes more accurately. This is because the brain can use the information from both eyes to create a sharper image.
- Reduced eye strain: Stereopsis can help to reduce eye strain by allowing the eyes to work together more efficiently. This is especially important for activities that require us to focus our eyes for long periods of time, such as reading or using a computer.
- Improved hand-eye coordination: Stereopsis is essential for good hand-eye coordination. This is important for activities such as sports, playing video games, and surgery.
Binocular Dysfunction
People with binocular dysfunction may experience problems such as:
- Difficulty judging distance: This can make it difficult to drive, walk, or play sports safely.
- Clumsiness: This can make it difficult to perform everyday tasks.
- Eye strain: This can make it difficult to focus on tasks for long periods of time.
- Amblyopia: This is a condition in which one eye is weaker than the other.
- Amblyopia can be caused by binocular dysfunction.
An example of a lack of understanding of binocular vision in Thailand is the popularity of mono vision LASIK. People get LASIK in one eye to see far and in the other eye to see near, so they don't have to wear glasses. However, this can lead to problems with binocular vision, such as double vision, headaches, and difficulty judging distance.
The author of the text argues that mono vision LASIK is a "Borneol in exchange for salt" - a trade-off that is not worth it. They say that losing stereopsis is a major loss, as it is essential for many everyday activities, such as driving, playing sports, and even eating.
The author also warns that mono vision LASIK is difficult to correct. If the patient is not happy with the results, they may need to wear glasses or contact lenses to correct the vision in one eye.
The author concludes by saying that binocular vision is a complex issue that is often overlooked. They argue that more education and research is needed to improve the understanding and treatment of binocular vision problems.
Here are some additional details from the text:
- The author says that many people who get mono vision LASIK are not aware of the risks involved. They are often lured in by the promise of being able to see clearly without glasses.
- The author says that mono vision LASIK can be difficult to adjust to. It can take months or even years for the brain to learn to fuse the two images from the two eyes.
- The author says that mono vision LASIK can lead to a number of other problems, such as eye strain, headaches, and dizziness.
The last
To my fellow optometrists,
If we are still only working on short-sightedness, long-sightedness, and astigmatism, and then promoting the sale of glasses, and demanding to be different from the opticians who are already working, then it is only natural to be disappointed. Only a madman would think that doing things roughly like everyone else would make them more important than anyone else simply because they have a piece of paper on the wall.
But if you really want to be dignified in the field of optometry, you must go deeper to the level of binocular function in order to be truly valuable to patients. Because we all know that incorrect vision can cause the function of the two eyes and the focusing system to malfunction.
We will not dare to arrange the vision, we will not dare to examine the vision incorrectly. Our work must not be rough. But if we don't know about binocular function, we will quickly do it roughly. 10-20 minutes to finish the exam, quickly sell and close the bill to receive a new case. (Optometry shops that hire optometrists to work often do this, quickly examine, quickly close the sale to open up new customers. I will tell you here that "Optometry work, the faster it is, the wronger it is”).
Working roughly is not wrong in legal terms (because there is no law), but in terms of professional ethics, it is considered wrong. And we must not forget that "law" is the most basic rule that the general public should have because good and evil are really common sense, but people have a lot of desires, so they pretend not to know which is right or wrong. Therefore, there must be laws to control those with thick desires. But ethics are rules for a higher mind. For example, drinking alcohol (at home) is not illegal, but drunk driving is illegal. But in terms of precepts (ethics), it is considered wrong from the moment you drink, even if you do not drive.
Therefore, optometrists with a 6-year diploma should not work as equals to just technicians. It is like a monk who is known to be virtuous and behaves like the morals of a householder. It would not be right. And if we can't even keep the Five Precepts, then there is no point in holding a book of merit and claiming to be virtuous.
Good and proper behavior does not need to be shouted or invented marketing words to attract attention from anyone. Because precepts (ethics) are in the practice, not in the book of merit (certificate). Because the value is created from the work we do.
So, let's think about it.
In summary, the author is urging optometrists to focus on binocular function in their work. They argue that this is the only way to truly be valuable to patients.
The author also criticizes optometrists who work roughly and promote the sale of glasses. They argue that this is not only unethical, but it is also not in the best interests of patients.
The author concludes by saying that optometrists should focus on their work and let their actions speak for themselves. They should not need to shout or invent marketing words to attract attention.
Thank you for your reading.
Dr.loft ,O.D.
Good Luck

Dr.Loft O.D.
578 ถ.วัชรพล ท่าแร้ง บางเขน กทม 10220
Mobile : 090-553-6554
Line id : loftoptometry
maps : LOFT OPTOMETRY MAPs
Product :
LINDBERG : rim Max, 48/23. Colour: 10 Temples: Wide, 145 mm, 10. Inner rim: K160
Rodenstock : Impression B.I.G. Norm 1.6 AllRound CMIQ3 ,w/ Solitare Protect Plus 2